Click on the button below to view more information
Welcome to the Quality Integration page! We are excited to offer you the latest information and resources in healthcare quality. On this page you will find information for all things Quality related including Organizational Leadership, Patient Safety, Process Improvement, and Hospital Resources to name a few. The intent is to provide a one stop shop so you no longer need to go several websites to gather information instead you can visit the Quality Integration page and find the resources you need. We are excited to be on this journey with you and provide the resources and the support you need to be successful in your role.
605-789-4995
Signup today to receive our free newsletter featuring all the most important healthcare news and events for South Dakotans.

© 2023 South Dakota Association of Healthcare Organizations
All rights reserved | Privacy Policy
Website designed by: | Chris Berke

Purpose of MBQIP: MBQIP is a quality improvement activity under the Federal Office of Rural Health Policy’s (FORHP) Medicare Rural Hospital Flexibility (Flex) grant program. Launched in 2011, the goal of MBQIP is to improve the quality of care provided in critical access hospitals (CAHs) by increasing quality data reporting by CAHs and then driving quality improvement activities based on the data. MBQIP provides an opportunity for individual hospitals to look at their data, compare their results against other CAHs, and partner with other hospitals around quality improvement initiatives to improve outcomes and provide the highest quality care to every patient. MBQIP/Flex program is brought to you by the SD Office of Rural Health. The SD Flex Coordinator is Terri Nihil. If you have questions on how this program is administered, please contact Terri at terri.nihil@state.sd.us.
Did you know that by participating in the MBQIP/Flex program, SD hospitals have received benefits such as:
Without your participation in MBQIP/FLEX, these programs and benefits would not be available.
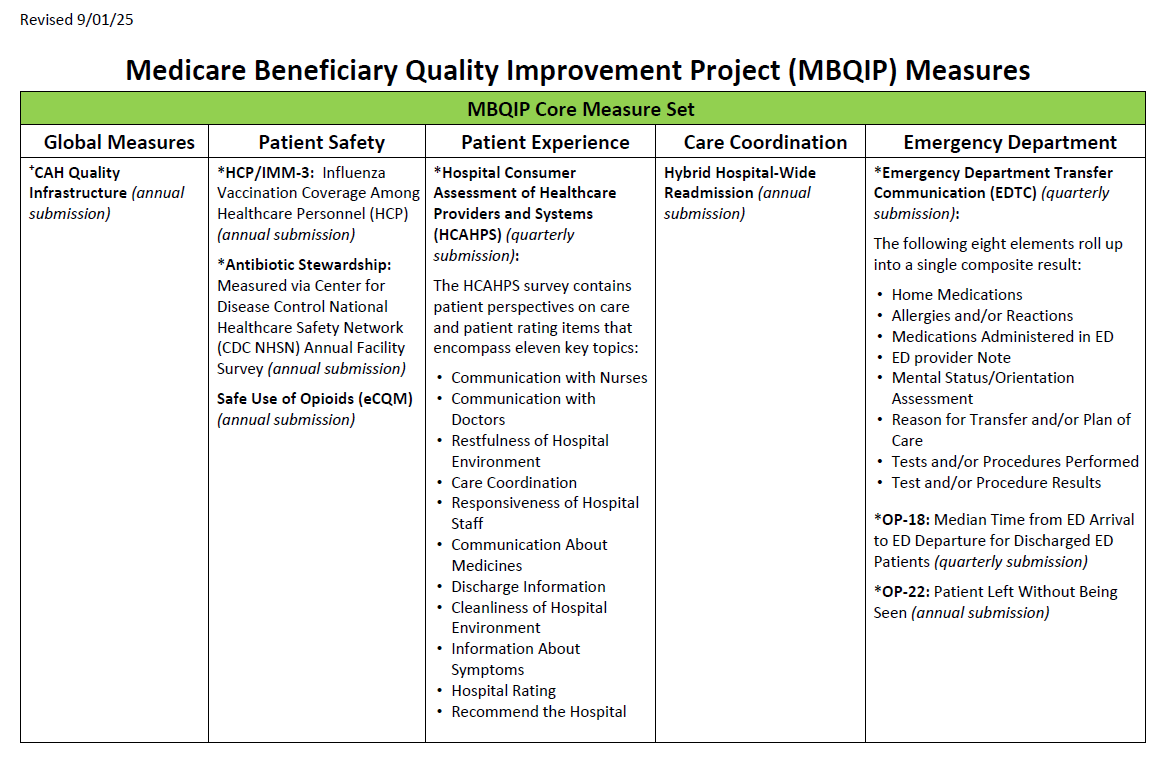
This table lists the core MBQIP Measure for South Dakota. There are 5 domains: Global Measures, Patient Safety, Patient Experience, Care Coordination, Emergency Department.
Below is information that will help to answer questions you may have or provide you with additional resources. If you are not finding the information you are looking for, please contact the SDAHO Quality Team by emailing Michelle Jury at Michelle.Jury@sdaho.org.
NEW Measure Exclusions for 2025 (page 2)
A Dive Into Emergency Department Transfer Communication (EDTC) | Courtnay Ryan, Telligen | Presentation | Video
Using your MBQIP Data Data Report to Inform Your Quality Improvement Project | Courtnay Ryan, Telligen | Presentation | Video
Psychological Safety | Molly Mackey, LEAderRNship Institute | Presentation
Surveyor Preparedness | Jean Koch, SD Dept of Health | PresentationFrom Compliance to Strategy: Positioning Quality as a Strategic Priority | Donna Gorby, Accreditation Commission for Health Care | Recording
Data that Moves People - Using Quality Data to Drive Leadership and Board Action | Donna Gorby, Accreditation Commission for Health Care | Recording
Telling the Quality Story, Helping Boards Understand Their Oversight Role | Todd Linden, FACHE, President, Linden Consulting, CEO Emeritus, Grinnell Regional Medical Center | Recording South Dakota Rural Health Swing Bed Series
When it comes to verifying OP-18 data submissions, only hospital staff with an active HARP account and appropriate access to HQR can run the reports necessary for verification. Here is a step-by-step guide to help: